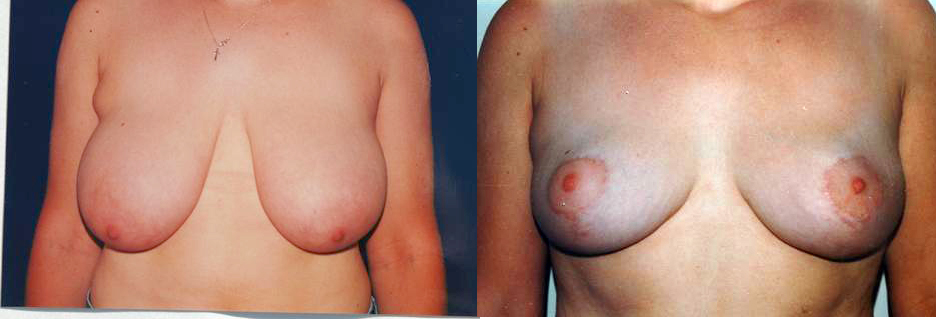
Breast reduction, or reduction mammoplasty is for a woman with very large, heavy breasts. The goal is to give the woman a more attractive contour with smaller, better-shaped breasts in proportion with the rest of her body. She will also benefit from easier fitting of clothing, lessening of back problems, an improved self-image and better and more comfortable exercise capability.
Medical problems associated with very large breasts caused by the excessive weight include back and neck pain, skin irritation, skeletal deformities and breathing problems. Bra straps may leave shoulder indentations. Large, heavy breasts also contribute to poor posture, and can interfere with normal daily activities such as exercise. Excessive breast size may also lead to a decreased sense of attractiveness and self-confidence. Breast reduction is sometimes covered by insurance. Our staff will assist you in obtaining preauthorization.
The Procedure
Breast reduction requires general anesthesia and usually is done as an outpatient. The surgery removes fat, glandular tissue, and skin from the breasts, making them smaller, lighter, and firmer. It can also reduce the size of the areola, (the darker skin surrounding the nipple). The result may be further enhanced by liposuction of the side of the chest and near the armpit. There are numerous variations in technique for this procedure. These variations alter the position of the incisions and subsequent scars, and how the nipple-areola is transferred to its new position.
Nipple preservation
Almost all breast reductions require preservation of the nipple blood supply and then transposing the nipple to a higher position. One exception is for women with extremely long large breasts that are extremely droopy. In order to move the nipple, the blood flow to the nipple must be preserved through a tissue connection (the pedicle). The preserved pedicle blood flow comes from one quadrant of the breast and the other quadrants are removed. All of these methods have nearly equivalent potential to provide adequate nipple blood flow when properly performed. The difference is the direction of the blood flow and where the excess breast is removed:
One exception is for women with extremely long large breasts that are extremely droopy breasts with the nipple as low as the belly button. These women may require removal of the nipple and then re-grafting in a higher position on the smaller breast.
Incision placement
There are many variations of incision placement that determines the position of the final scar and the shape of the breast. With all variation a part of the incision is made as a circle around the nipple-areola in order to move the nipple to a higher position. The remainder of the incision is used to remove excess skin. The most common variation are the Vertical scar with a medial or lateral pedicle, the Wise pattern with an inferior pedicle and the Benelli technique with a periareolar scar. My personal preference is the vertical incision with a medial pedicle. However, in certain patients other techniques may be used.
Benelli (donut, periareolar)
- The scar forms a circle around the areola, but there is a tendency for the scar around the nipple to widen
- This technique can only be used for very minimal reductions and is most commonly used for lifting the breast (mastopexy) rather than reducing the size of the breast
- This technique tends to make the breast flatter, rounder and less projecting
Wise pattern (anchor shape)
- The incision goes around the nipple and then down to the breast crease and then horizontally medially and laterally in the crease.
- This had been the most common technique for many decades until recently when the vertical scar technique was introduced.
- The scars at the innermost and outermost edges may be heavy and noticeable.
- This technique sometimes leads to breast “dropdown”. The breast becomes excessively full in the lower part of the breast and hollowed in the top part. If this occurs the nipple points upward.
Vertical Scar (LeJour or Findlay-Hall)
- With this technique the scar is around the nipple and then extends down to the breast crease (no scar is made horizontally in the crease)
- With this technique the skin bunches at the inferior aspect creating bunching under the breast. However, most of this spontaneously shrinks over 6 months.
- Occasionally a small office revision with local anesthesia is required to remove bunching skin that does not completely shrink
- The vertical technique gives a more conical projecting breast then the other techniques.
Breast reduction typically produces a high level of patient satisfaction. It ends the physical discomfort of overly large breasts; makes your body appear more evenly proportioned, and clothes fit better. As much as you desired the change, your new image will take some getting used to. Give yourself — and your family and friends — time to adjust to the new you and, like most women, you will enjoy the benefits.